Latifa Tower 18th floor – 1806,
Sheikh Zayed Road,
Trade Center 1,
Dubai
United Arab Emirates
Say Goodbye to Psoriasis, Hello to Confidence.
Psoriasis Treatment
Scroll Down
Psoriasis
Say Goodbye to Psoriasis , Hello to Confidence.
Psoriasis
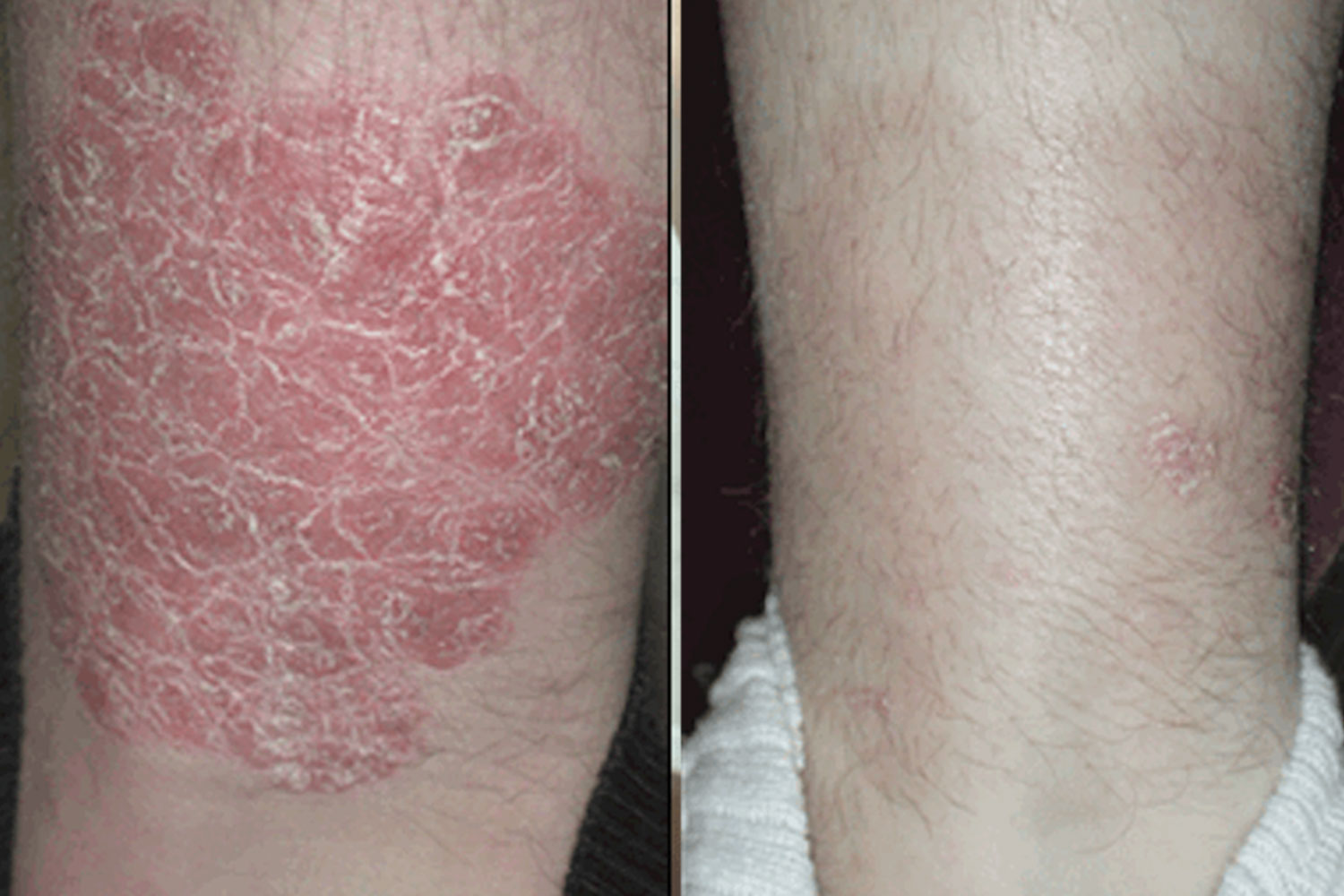
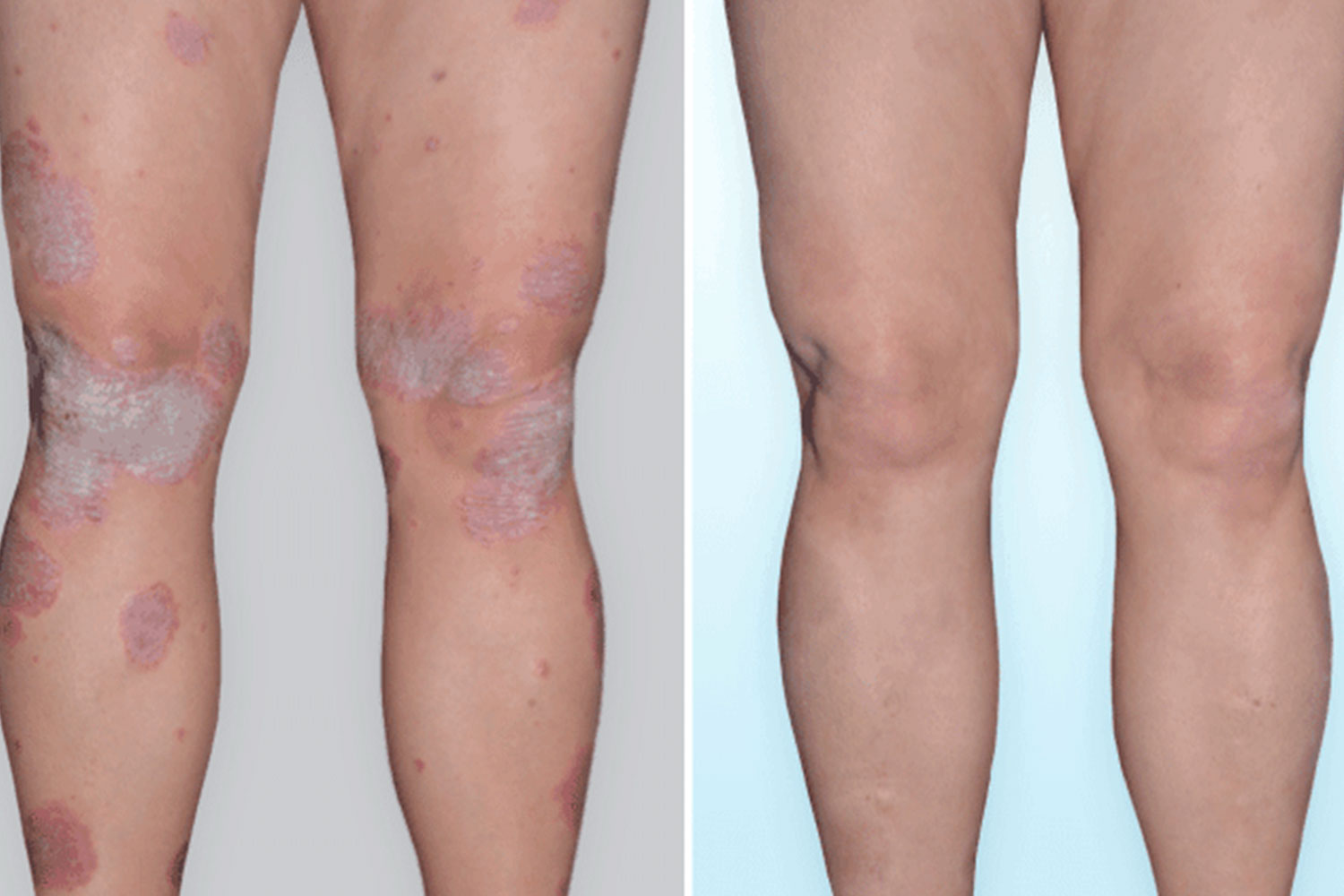
Psoriasis is a chronic, immune-mediated inflammatory skin disorder marked by abnormal keratinocyte proliferation and differentiation. It is primarily driven by an interplay between genetic predisposition, environmental triggers, and immune system dysregulation. The pathogenesis involves the activation of dendritic cells and T-helper (Th) cells—especially Th1, Th17, and Th22 subtypes—which secrete pro-inflammatory cytokines such as TNF-alpha, interleukin (IL)-17, IL-23, and IL-22. These cytokines stimulate keratinocytes to proliferate rapidly and produce inflammatory mediators, further amplifying the immune response in a self-perpetuating loop.
The result is excessive and rapid turnover of skin cells, which accumulate and manifest as thickened, erythematous plaques covered with silvery-white scales—hallmark features of psoriasis. The stratum corneum retains nuclei (parakeratosis), while the stratum granulosum is diminished or absent. Vascular changes such as capillary dilation in the dermal papillae contribute to erythema and pinpoint bleeding when scales are removed (Auspitz sign).
Psoriasis also affects other tissues. Nail involvement is common, presenting as pitting, onycholysis, or subungual hyperkeratosis due to matrix and nail bed inflammation. In some patients, the inflammatory process extends to the joints, resulting in psoriatic arthritis—a seronegative spondyloarthropathy that may cause pain, stiffness, and joint deformities.
Triggers for psoriasis flare-ups include infections (e.g., streptococcal pharyngitis), stress, cold weather, certain medications (e.g., lithium, beta-blockers), trauma to the skin (Koebner phenomenon), and lifestyle factors such as smoking and alcohol consumption.
Overall, psoriasis is not merely a skin condition but a systemic disorder with multi-organ involvement, requiring long-term management to control inflammation, reduce flare frequency, and improve quality of life.
Self-help :
1. Keep skin hydrated with thick emollients
Regular use of rich moisturizers helps lock in moisture, soothe dryness, and support the skin barrier.
2. Use tar or salicylic acid shampoos for scalp involvement
These medicated shampoos reduce scaling, itching, and inflammation in scalp psoriasis.
3. Avoid known triggers (e.g. stress, alcohol, smoking)
Identifying and minimizing personal triggers can help prevent flare-ups and keep symptoms under control.
4. Maintain a healthy weight and lifestyle
A balanced diet, regular exercise, and weight management reduce systemic inflammation and improve treatment response.
Medical Management :
Topical: Corticosteroids, calcipotriol, coal tar, tazarotene These are applied directly to the skin to reduce inflammation, slow skin cell growth, and relieve itching and scaling.
Systemic: Methotrexate, cyclosporine, acitretin Oral or injectable medications that work throughout the body to control moderate to severe psoriasis by suppressing the immune response.
Biologics :
Targeted therapies that block specific immune pathways involved in psoriasis, effectively reducing inflammation and skin lesions in moderate to severe cases.
TNF inhibitors (etanercept, adalimumab) Biologic drugs that block tumor necrosis factor-alpha (TNF-α), a key inflammatory cytokine involved in psoriasis.
IL-17 inhibitors (secukinumab) Target interleukin-17 to reduce inflammation and plaque formation in moderate to severe psoriasis.
IL-23 inhibitors (guselkumab) Block interleukin-23 to interrupt the inflammatory cascade and provide long-term psoriasis control.
New treatments :
Oral targeted therapy that blocks the TYK2 enzyme involved in immune signaling, helping reduce inflammation and plaque formation in moderate to severe psoriasis.
Phototherapy :
Psoriasis – Phototherapy: NB-UVB, PUVA Light-based treatments that slow skin cell growth and reduce inflammation; NB-UVB uses narrowband UVB rays, while PUVA combines UVA light with a photosensitizing agent (psoralen) for enhanced effect.